Neuroscience Overview
The scope of neuroscience has now broadened to include any systematic scientific experimental and theoretical investigation of the central and peripheral nervous system of biological organisms. The empirical methodologies employed by neuroscientists have been enormously expanded, from biochemical and genetic analysis of dynamics of individual nerve cells and their molecular constituents to imaging representations of perceptual and motor tasks in the brain. Many recent theoretical advances in neuroscience have been aided by the use of computational modeling.
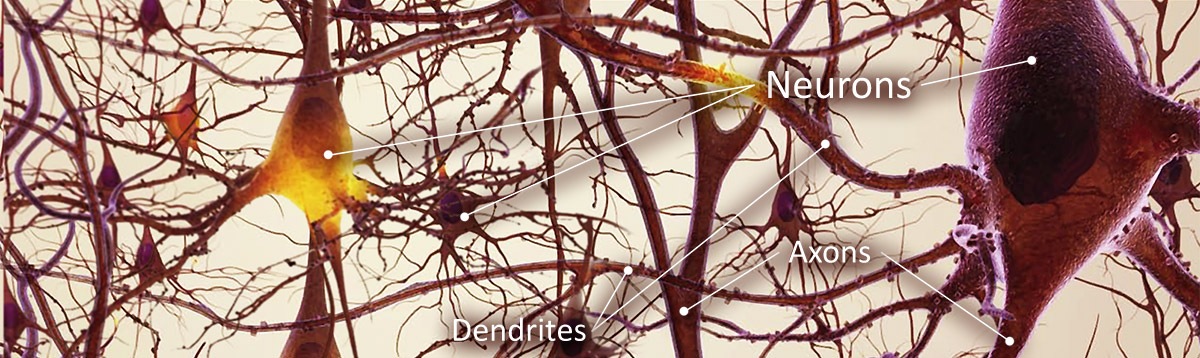
The nervous system is composed of a network of neurons and other supportive cells (such as glial cells). Neurons form functional circuits, each responsible for specific tasks to the behaviors at the organism level. Thus, neuroscience can be studied at many different levels, ranging from molecular level to cellular level to systems level to cognitive level. At the systems level, the questions addressed in systems neuroscience include how the circuits are formed and used anatomically and physiologically to produce the physiological functions, such as reflexes, sensory integration, motor coordination, circadian rhythms, emotional responses, learning and memory, et cetera. The related field of neuroethology, in particular, addresses the complex question of how neural substrates underlies specific animal behavior.
At the cognitive level, neuroscience addresses the questions of how psychological / cognitive functions are produced by the neural circuitry. The emergence of powerful new measurement techniques such as neuroimaging (e.g.,fMRI, PET, SPECT), electrophysiology and human genetic analysis combined with sophisticated experimental techniques from cognitive psychology allows neuroscientists and psychologists to address abstract questions such as how human cognition and emotion are mapped to specific neural circuitries. Neuroscience is also beginning to become allied with social sciences, and burgeoning interdisciplinary fields of neuroeconomics, decision theory, social neuroscience are starting to address some of the most complex questions involving interactions of brain with environment.
Methods employed in cognitive neuroscience include experimental paradigms from psychophysics and cognitive psychology, functional neuroimaging, electrophysiological studies of neural systems and, increasingly, cognitive genomics and behavioral genetics. Clinical studies in psychopathology in patients with cognitive deficits constitute an important aspect of cognitive neuroscience.
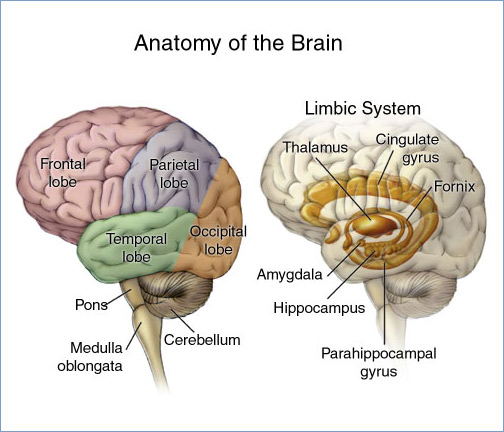
Cognitive Neuroscience is particularly relative to the study of Dementia realated diseases such as Alzheimers Disease. Alzheimer's is characterised by symptoms like loss of memory, loss of language skills and impairments in skilled movements. Additionally other cognitive functions such as planning or decision-making which are connected to the frontal and temporal lobe can be reduced. The correlation between memory and language in this context is very important because they work together in order to establish conversations. When both are impaired, communication becomes a difficult task.
Scientists believe that long before the first symptoms appear nerve cells that store and retrieve information have already begun to degenerate. There are two theories giving an explanation for the causes of Alzheimer's disease. The first describes plaques as protein fragmens which defect the connection between nerve cells. They arise when little fragments release from nerve cell walls and associate with other fragments from outside the cell. These combinded fragments, called plaques, append to the outside of nerve cells and destroy the connections. Then the nerve cells start to die because they are no longer provided with nutrients. As a conclusion the stimuli are no longer transferred. The second theory explains that tangles limit the functions of nerve cells. They are twisted fibers of another protein that form inside brain cells and destroy the vital cell transport made of proteins.
Neuropsychological studies show that cognitive deficits associated with the Alzheimer's disease (AD) are distinct from age-associated cognitive decline. Quantitative and qualitative differences are apparent across many cognitive domains, but are especially obvious in episodic memory (particularly delayed recall), semantic knowledge, and some aspects of executive functions. The qualitatively distinct pattern of deficits is less salient in very old AD patients than in younger AD patients. Although decline in episodic memory is usually the earliest cognitive change that occurs prior to the development of the AD dementia syndrome, asymmetry in cognitive abilities may also occur in this "preclinical" phase of the disease and predict imminent dementia. Discrete patterns of cognitive deficits occur in AD and several neuropathologically distinct ageassociated neurodegenerative disorders. Knowledge of these differences helps to clinically distinguish among various causes of dementia and provides useful models for understanding brain-behavior relationships that mediate cognitive abilities affected in various neurodegenerative diseases.
For more information on Alzheimer's disease and the role of Cognitive Neuroscience in its treatment and diagnosis, visit our Medivision web portal at alzheimersdisease-info.com
Studies often concentrate on Neurodegenerative diseases such as Motor Neuron Disease (MND; Amyotrophic Lateral Sclerosis, ALS), Parkinson's disease and related disorders, epilepsy, peripheral nerve disorders, and increasingly on acute brain injury including stroke and traumatic brain injury.
A primary tool used in clinical neuroscience studdies is Electroencephalography (EEG), the measurement of electrical activity produced by the brain as recorded from electrodes placed on the scalp. In some cases, such as epileptic studies, deeper brain activity cannot be recorded accurately or not at all by scalp EEG. Clinicians then use an invasive form of EEG known as intracranial EEG (icEEG) where electrodes are placed directly inside the skull. In some cases, a grid of electrodes is laid on the external surface of the brain, on dura mater yielding epidural EEG but in other cases, brain activity is recorded using deeper electrodes known as subdural EEG (sdEEG) and electrocorticography (ECoG). Because of the filtering characteristics of the skull and scalp, icEEG activity has a much higher spatial resolution than surface EEG. The technique is sometimes also referred to as stereotactic EEG (stereo-EEG or sEEG) to emphasize that it records from precise 3D locations defined by stereotaxy. However, since icEEG uses macro-electrodes for recording it can not detect single-neuron activity as it is feasible with neural implants based on micro-electrodes.
A routine clinical EEG recording typically lasts 20-40 minutes. During this time, it is common to perform different "activation procedures" which may evoke different activity than is seen during the resting awake state. These activation procedures include sleep, intermittent photic stimulation with a strobe light, hyperventilation and eye closure. When a routine EEG is done in a patient with suspected or known epilepsy, often it is to look for interictal discharges (i.e., abnormal activity resulting from "brain irritability" that shows a possible predisposition to epileptic seizures).
There are a number of benefits to using EEG in neuroscience research. One is that EEG is non-invasive to the research subject. Furthermore, the need for the subject to hold still is perhaps less stringent than in functional magnetic resonance imaging (fMRI). Another benefit is that many applications of EEG record spontaneous brain activity, and the subject does not need to be able to cooperate with the research (e.g., as is necessary in the behavioral testing of neuropsychology). Also, EEG has a high temporal resolution compared to techniques such as fMRI and is capable of detecting changes in electrical activity in the brain on a millisecond time scale. Much of the cognitive research conducted with EEG uses the event-related potential (ERP) technique. Most ERP paradigms involve a subject being provided a stimulus to react to either overtly or covertly. There are often at least two conditions that vary in some manner of interest to the researcher. As this stimulus-response is going on, an EEG is being recorded from the subject. The ERP is obtained by averaging the EEG signal from each of the trials within a certain condition; averages from one stimulus-response condition can then be compared with averages from the other stimulus-response condition(s).
Educational programming for healthcare professionals
MEDIVISION ™ collaborates with recognized leaders in the fields of medical and pharmaceutical sciences to provide educational programming for medical specialists, universities and medical schools. Our DVD catalog contains over 200 titles in 35 separate healthcare fields, including a wide variety of specialist topics essential to healthcare professionals.
Neuroscience programming >